
|
About the presenter: Vivian Sisskin is an instructor and clinical supervisor in the department of Hearing and Speech Sciences at the University of Maryland, and was awarded the 2008 Excellence in Teaching Award by the College of Behavioral and Social Sciences. She is an ASHA Board Recognized Specialist in Fluency Disorders and serves as Coordinator for ASHA's Special Interest Division 4, Fluency and Fluency Disorders. She has authored articles and continuing educational materials related to the treatment of stuttering in school-age children. In addition to assessment and treatment, her workshops include strategies for effective group therapy and supervision in the areas of fluency disorders. Vivian is a private practitioner in the Washington D.C. area. |
The Problem of Stuttering: A Visual Aid for Counseling
by Vivian Sisskin
from Maryland, USA
Purpose of the Chart:
I use the attached chart in the course of counseling older children, teens, and adults who stutter, as well as those in their circle of support (family members, teachers & friends). It increases understanding of stuttering as a communication disorder, rather than simply a speech disorder. It demonstrates that the severity of the stuttering problem is a product of not only the frequency of disfluency and the appearance of struggle, but also (1) the time and energy thinking about what others will think, and (2) the feelings associated with both thoughts and actual struggle during communication.
What the Columns Represent:
The columns are based on the ABC's of Stuttering (Cooper, 1985), where "A" represents the affective components of the problem, "B" represents the behavioral aspects, and "C" represents the cognitive aspects of the problem. When explaining this to people who stutter (PWS) and their supporters, I might include the following terminology, adjusted for the developmental level of my younger clients: Affective - the feelings and emotions related to stuttering; what you feel in your gut or in your heart. Behavioral - The things you do, or have done in the past, to cope with stuttering. These behaviors might have been a way to hide stuttering, a response to frustration, or advice that someone gave you that "worked", at least initially. They have now become part of the problem. Cognitive - What you think before, during or after you stutter. These may be worries, directives, or predictions.
A Tour of the Columns:
What PWS "DO". . . .
I begin with behaviors because they are the most concrete. I also find that this helps to de-mystify the problem of stuttering quickly because PWS realize that their particular pattern of struggle is not necessarily dictated by genetics or neurology. In fact, the aspects of their stuttering that create most of the problem may be those that have been learned, and they can learn new ways of behaving. I might say, "You may not have a choice as to whether or not you stutter, but you do have a choice as to whether or not you struggle". I might take the opportunity to describe how secondary behaviors may be learned through negative reinforcement in an operant model (Brutten and Shoemaker, 1967), drawing some pictures and demonstrating with analogies. I might describe how an interjection such as "um", which has become a distracting linguistic escape behavior, might have first begun with an innocent use of a filler to "buy some time" in the moment of fear. Its powerful reinforcement as an escape from the stuttering block resulted in a conditioned response that has been practiced for many years.
What PWS FEEL . . . .
This follows logically because the escape/avoidance behaviors described above were motivated in an attempt to prevent negative feelings, particularly shame and embarrassment. However, for younger children, the escape behaviors are often motivated by preventing frustration (increasing efficiency) rather than shame, and often quite subconsciously. I sometimes probe to help the client identify the feelings most often triggered by struggle, by having them complete the sentence, "When I struggle more than I can tolerate, I feel _____".
What PWS THINK . . . .
Talking about this aspect of the stuttering problem is the most enlightening for those who can be covert to the outside world, and particularly for their supporters who do not see the problem. However, just about all PWS have a good dose of this column in their profile. This refers to the constant negative self-talk that has become automatic when confronted with a speaking situation, or a potential speaking situation. The thoughts are different from feelings, as they can be put easily into words, and often begin with, "He'll think ____", "They won't ____", & "I can't ____".
I might probe clients to identify some of their maladaptive thoughts by inviting them to complete the following sentence, "If I show "ugly" stuttering, people will think _______", or "If he knows that I stutter, then ______".
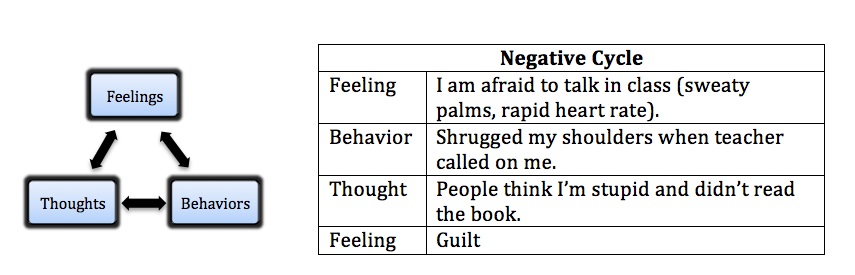
Positive and Negative Spirals:
The three columns form a dynamic model with each area impacting the other two. The vicious cycle can begin with any of the three areas. Examples below:

Implications for Treatment:
The problem profile can inform the treatment plan:
There is great variability among clients in terms of the relative proportion of life impact from each of the three areas. Through counseling and discussion, clients and clinicians can agree upon shared goals that are both functional and meaningful to the client.
The problem profile can help to explain treatment rationales and promote change:
When clients understand why an objective or therapy strategy is introduced in treatment, independent problem solving is more likely, both in choices made outside of therapy and in independent assignment development. If a therapy target for desensitization is chosen, for example - asking a question in a store, the client can also identify a positive cycle in advance that is realistic and promotes change.

Resources:
- Brutten, G.J. & Shoemaker, D.J. (1967). The Modification of Stuttering. Englewood Cliffs, NJ: Prentice Hall.
- Cooper, E.B. & Cooper, C.S. (1985). Cooper Personalized Fluency Control Therapy-Revised. Allen, TX: DLM Teaching Resources.
SUBMITTED: September 4, 2011
Return to original language with "show original" button at top left.