
|
About the presenter: Larry Molt is chair of the Department of Communication Disorders and the director of the Neuroprocesses Research Laboratory at Auburn University. He holds a dual masters degree in speech-language pathology and audiology from the University of South Florida and Ph.D. in speech and hearing science from the University of Tennessee. Larry is an ASHA Board-Recognized Fluency Specialist. Larry was named 2003 Speech-Language Pathologist of the Year by the National Stuttering Association. His current research involves EEG topographic mapping of brain activity in a variety of speech, language and auditory disorders, with a prominent interest in stuttering. |
A Brief Historical Review of Assistive Devices for Treating Stuttering
by Larry Molt
from Alabama, USA
The purpose of this paper is to introduce the reader to a variety of anti-stuttering devices that have been used to treat stuttering. What follows is by no means an exhaustive list of all such devices. Rather, a few examples of each of the different classes of devices are presented. Neither is an extensive review of the literature surrounding the devices included, for that would have resulted in a massive paper, beyond the acceptable format for the ISAD conference, A sampling of references is included, with an emphasis on seminal articles for each category of device. The author apologies in advance for omission of particular devices or particular articles that may be "favorites" of some of the readers.
Introduction
The use of devices to cure, or at least control, stuttering is not new. One of the earliest historical references to anti-stuttering treatment devices are those employed by the famous Greek orator and statesman, Demosthenes (384-322 B.C.). Demonsthenes, reportedly a stutterer, overcame his speech impediment by practicing orating in several different conditions: with pebbles in his mouth, against a loud background noise (crashing surf), and while climbing steep hills (heavily laden with leaden plates hung over his shoulders). While clearly somewhat primitive in nature, Demonsthenes' ideas for anti-stuttering treatment devices seem remarkably similar in purpose to devices in use today, i. e., such as those employed for changing articulatory kinematics, respiratory dynamics, and other production characteristics. A variety of devices have been utilized, with a variety of purposes. Table 1 provides a summary of general categories of assistive and anti-stuttering devices. Some devices are aimed at forcing the person who stutters

to change the manner in which they speak. Others are utilized to provide the client with more easily observable feedback of their current physiologic status or production pattern, often to assist them in achieving speech production targets utilized in therapy. Still others alter the natural feedback the client receives in an attempt to prevent stuttering.
Types of Assistive and Anti-Stuttering Devices
Devices That Alter Speech Motor Production Patterns
Anyone who stutters or works with individuals who stutter is aware of a variety of curious and fascinating phenomenon about the disorder. One of the more peculiar features observed with the disorder is that many stuttering individuals can temporarily achieve a high degree of fluency simply by changing their speech production pattern. Talking faster or slower than normal, talking in a sing-song pattern, in a softer voice or a louder voice, talking with a monotone and/or monoloudness pattern, talking with a raspy voice (vocal fry) are just a few examples of altered speech patterns that may induce temporary fluency. Over the years, many inventors have taken advantage of this particular phenomenon to create anti-stuttering devices that force the user to mechanically alter their speech production pattern. Descriptions of several different types of these devices can be found in books by Charles Van Riper (1979) and Marcel Wingate (1997).
One of the earliest recorded devices of this type was invented by Jean Marie Itard, a French physician. Itard felt stuttering resulted from spasmodic weakness of the tongue and laryngeal muscles. He developed a series of strengthening exercises and he utilized a gold or silver "fork" placed under the tongue to hold it in a higher position in the oral cavity. While Itard's Fork and exercises did not result in a lasting cure of stuttering, his 1817 book "Mémoire sur le Bégaiement" (Memoir of Stuttering) may be one of the earliest books written on the disorder. Itard was also famous for his writings on human intelligence and his efforts at developing hearing aids and instruments for otologic surgery.
A second example is the Freed Stammercheck device. Patented in 1955, the Stammercheck consisted of a metal band that fit between the upper lip and the top of the gingiva, following along the gum-line, with two hook-shaped projections extending inferiorly near the first molars, ending just below the molar. Drawings of the Stammercheck device appear below. A rubber band was stretched between the two hooks, crossing the oral cavity and keeping the tongue dorsum from assuming its normal position inside the palatal vault. Wearers were forced to speak with a limited range of lingual movement, and the altered articulatory pattern also tended to slow the speech rate down.


A third device, the Bates Appliance (patented in 1851) was much more complex, designed to deal with various "forms" of stuttering. Shown in drawings from its 1851 patent application below, it consisted of three parts. These included a metal plate that fastened to the roof of the mouth (via wires around upper teeth) which protruded forward between the lips, keeping the lips apart and discouraging disfluencies on bilabial phonemes. Another piece consisted of a hollow tube, attached to the teeth with a rubber band that protruded between the lips, to release impounded air pressure to prevent stuttering on "dental" phonemes. The third piece was a "laryngeal compressor", a leather collar that was worn around the neck, used to prevent stuttering on "guttural" (voiced) phonemes. The compressor, and the pressure it exerted against the larynx, could be controlled by either the buckle or by a pressure plate in front that could be moved deeper or shallower via a thumbscrew arrangement. Potter (1882) described his own experiences with the $35.00 device (a rather princely sum in those days), which yielded encouraging initial success but the effects quickly wore off.

A fourth example of devices aimed at inducing a forced alteration of speech production is the Idehara "Stutter-Cure" appliance. The Idehara appliance (shown below) consisted of a palatal prosthesis similar to that of a modern acrylic orthodontic retainer, fitting along the interior dental bite wings and sitting against the hard palate. A protruding center bulge housed a whistle and, on its inferior surface, a sharp pin projecting downwards into the oral cavity. The whistle was used to encourage continuous airflow when speaking, Theoretically, the whistle could only be heard by the speaker, and the speaker was instructed to keep the whistle going throughout the utterance. The pin was used to keep the wearer from placing the tongue too close to the roof of the palate, forcing the adoption of a lower tongue carriage when speaking.

Physiology and/or Production Feedback Devices
A second class of devices that has been used in the treatment of stuttering are those providing visual and/or auditory feedback on the user's (speaker's) current physiological state or speech production patterns. Typically these types of devices have been used to aid the client in identifying and altering speech production processes as part of therapy A variety of devices have been employed over the years, and can be categorized to a certain extent either by the specific physiological processes that are targeted, or by the type of feedback provided (auditory, visual, or somatosensory). Examples of physiological process that have been targeted include attempts to provide feedback on respiratory kinematics, muscular tension in phonatory or articulatory structures, duration of phonatory and or articulatory production, or other aspects of phonatory or articulatory timing.
Respiratory Kinematics
Many individuals who stutter show evidence of disruptions in their respiratory patterns. Bloodstein (1995) indicated these respiratory irregularities include "antagonisms between abdominal and thoracic breathing, irregularity of consecutive respiratory cycles, prolonged expirations or inspirations, complete cessation of breathing, interruptions of expiration by inspiration, and attempts to speak on intake of air". These are so common and conspicuous that respiratory irregularities were not only among the earliest factors to be examined as a possible cause of stuttering, but were also early targets as speech production processes to alter in therapy in helping the client achieve a higher degree of fluency (e. g., Lewis' 1897 "Phono-Metric Institute and School for Stammerers"). In the earlier description of the Idehara "Stutter-Cure" device (above) it was noted that one component of the device, the whistle, was utilized to encourage a constant and consistent airflow.
An example of a device used to provide feedback on respiratory kinematics is the "Breathing Monitor", a type of induction plethysmograph, that was included in the "Dr. Fluency", computerized stuttering treatment program (Friedman, Fetterman, and Jolson, 1999). The breathing monitor consists of 2 elastic straps (belts), one worn around the chest, and a second worn around the abdomen, which are connected to a computer and the Dr. Fluency software via a hardware interface component (the breathing monitor "box"). In the photograph of the Dr. Fluency system (below), the belt is laid out at the bottom of the picture, with the interface box directly above it. A strain gauge (a measurement sensor whose electrical resistance is altered as it is stretched) is enclosed inside the center portion of each elastic belt. As the individual breathes, the belt around the chest or the abdomen is stretched, altering the electrical signal from the strain gauge.
The breathing monitor was used to provide the client with real-time feedback on obtaining adequate respiratory intake, the relative use of abdominal vs. thoracic (chest) breathing patterns, and breathing cycle coordination with speech patterns. The training began with general breathing activities (unaccompanied by speech) moving to coordination of speech and breathing first in single sounds, the multisyllabic words, phrases, and finally into passage-length material. Other therapy programs have utilized similar devices. The CAFET (Computer Aided Fluency Establishment Trainer) therapy program (Goebel, 1994) provides a respiratory monitor for feedback on respiratory kinematics as part of the program's training regimen. The Precision Fluency Shaping Program (PFSP; Webster, 1980) was the precursor to today's Hollins Fluency System. The PFSP initially made use of two separate feedback instruments in it's intensive therapy program: a "Voice Monitor" which provided acoustic analysis of sound/speech onset, loudness, and duration, and a "Respiration Monitor", which used an abdominal induction plethysmograph strap which provided feedback on respiratory kinematics.


Phonatory and Articulatory Kinematics
Both phonation and articulation are other speech production processes that often appear to function abnormally in many people who stutter. Consequently, as was seen with respiration, both have received considerable attention as a possible source of stuttering, as well as a target for modification in many therapy approaches. These include attempts to encourage the use of a gentle onset of phonatory activity, sustained phonation, and attempts at reducing muscular tension (hypertonicity) in phonatory and or articulatory muscles, via electromyographic (EMG) biofeedback.
Devices used to train gentle/gradual phonatory onset: Several therapy programs utilize electronic analyses and feedback of acoustic speech characteristics. The programs listed in the respiratory monitoring devices section of this paper (Precision Fluency Shaping Program/Hollins Fluency System, CAFET, and Dr. Fluency) all utilize acoustic monitoring devices. The PFSP "Voice Monitor" is a good example of an early acoustic monitoring device. The voice monitor (pictured below) consisted of the analysis and feedback unit and a microphone. The device provided immediate feedback of voice onset patterns, duration, and amplitude/loudness. As each speech production target was introduced to the client, they received training on the type of feedback from the voice monitor that indicated correct achievement of the target. Once the clinician was sure the client knew what to look for on the voice monitor, the client could practice without the clinician's presence, freeing up the clinician while the client engaged in intensive practice on their targets. Today's version of the PFSP, the Hollins Fluency System, uses personal computer-based hardware and software to replace the voice monitor. The software program also presents the stimuli (sounds, words, and longer utterances) to practice for each target, data on performance over time, and an opportunity for the client to self-judge the accuracy of their production before feedback is given. Similar computer-based devices are provided by the Dr. Fluency program (Speech Therapy systems, Ltd.: Friedman, Fetterman, and Jolson, 1999) and the CAFET (Computer Aided Fluency Establishment Trainer) therapy program (Goebel, 1994), among others.


Devices used to train sustained phonation: One of the production targets in the Shames and Florance (1980) Stutter-Free Speech Program was sustained phonation, sometimes referred to as continual phonation. In search of a more effective method for teaching sustained phonation, George Shames, in conjunction with William Torgeson, developed a "Vocal Tactile Feedback Method and Associated Apparatus" (US Patent 4685448, 1987). The device was originally marketed as the Vocaltech personal vibrotactile feedback device (PVFD). The unit fit into a shirt or pants pocket, with the vibrotactile apparatus worn around the neck, provided a vibrating sensation as its feedback modality. The unit was developed to help those individuals who have a difficult time sensing whether or not they are maintaining a continuous phonation pattern. As long as the individual maintained a sustained phonation speaking pattern, the vibration continued, so clients were instructed to "keep the vibration going throughout your utterance".I

In recent years, Shames, in conjunction with CAJE Enterprises, has altered the device to provide transcutaneous electrical nerve stimulation (TENS), rather than vibratory feedback. The device now consists of the pocket sized processing unit, a lapel microphone, self-adhesive gel pad TENS electrodes, and a set of headphones which can be used to provide an optional delayed auditory feedback signal (DAF). Speech is picked up by the lapel microphone, delayed from 15ms to 150ms, amplified, and delivered to the TENS electrodes. The electrodes provide a mild electrical shock to the skin, in the form of a "tingling" sensation, whose strength can be adjusted. According to Dr. Shames, the use of TENS feedback results in less adaptation and hence greater awareness of the use of sustained phonation than seen with vibrotactile feedback. Known as the EZ-Speech Sustained Phonation Unit (SPU), it is distributed through EZ-Speech, Inc. in Chester, VA.
Devices to reduce phonatory and/or articulatory tension: In the 1970s, as biofeedback approaches for treating a variety of disorders first appeared (Basmajian, 1972), interest among stuttering researchers and clinicians immediately turned to this new approach to managing physical behaviors. Guitar (1975), Hanna, Wilfling, & McNeil (1975), Cross (1977), and Lanyon (1977) provided some of the earliest research on the use of EMG biofeedback in treating stuttering. In biofeedback, sensors are used to pick up physiologic signals or activity (EMG activity, temperature, sweat or other body moisture, pressure, etc.) that may be too subtle for the individual to consciously detect. The biofeedback device amplifies the signal, and provides a feedback signal that indicates current physiologic status and any change in the signal (such as an increase or decrease in EMG activity). The feedback may be in a variety of forms -- visual (e. g., needle movements on a meter or increasing or decreasing light intensity or number of lights on an LED display), auditory (change in pitch of a continuous tone or in click rate), or combinations of modalities. The feedback allows even extremely subtle changes in physiologic status to be monitored, with the hope that use of biofeedback will allow the individual to gradually learn voluntary control over the activity.
For EMG biofeedback, electrodes are attached to the skin surface (overtop of the muscle or muscles of interest). The electrodes pick up electrical activity at the myoneural junction, as the electrochemical discharges from the nerve fibers cause the muscle fibers to contract. In general, an increase in muscle tension (contraction) is marked by an increase in the EMG signal, so EMG provides a grossly approximate indication of current muscle contraction/tension. Since stuttering often is associated with excessive muscle tension in respiratory, phonatory, and/or articulatory structures, EMG biofeedback offered a unique way to train reduced muscle tension, hopefully facilitating more fluent speech production. The aforementioned studies experimented with EMG biofeedback from a variety of structures, including laryngeal area (Hanna et al., Guitar, Cross), lip (Guitar), jaw (Lanyon), and multiple sites (Guitar). All reported reduction in muscle tension and frequency of stuttering.

Other biofeedback devices have been used in an effort to reduce phonatory tension as it is evidenced acoustically, rather than electromyographically. Casa Futura Technologies (www.casafuturatech.com), a manufacturer and retailer for a variety of assistive stuttering devices, recently introduced a "Vocal Tension Biofeedback" analyzer that is a component in the company's "Pocket Speech Lab". The pocket speech lab is primarily an altered auditory feedback (AAF) device and is discussed elsewhere in this article. The vocal tension biofeedback component offers real-time analysis of frequency and amplitude aspects of the speaker's voice that the manufacturer feels are characteristic of excessive vocal effort and tension. The device provides visual (red light for excessive tension, green for appropriate tension) feedback and can also be set to provide negative feedback, switching on the AAF components when excess tension is detected, and cutting the AAF off when tension returns to appropriate levels. The manufacturer suggests that this may provide a system for "weaning" the speaker off of the need for AAF when speaking (if the user successfully minimizes vocal tension, fluency should be facilitated, and AAF will not be needed). Devices that examine acoustic phonatory onset patterns may also indirectly provide feedback on phonatory tension, although that is not their primary function.
Pacing/Timing Devices
Researchers, clinicians, and people who stutter have long been aware that speaking to a superimposed rhythm can facilitate a noticeably more fluent speaking pattern in many individuals who stutter. The commercial "stammering schools" that proliferated at the end of the 19th century, such as the Bogue Institute (Bogue, 1919) and the Lewis Phono-Metric Institute (Lewis, 1897) all capitalized heavily on rhythmic speaking techniques as an important component of therapy. Perhaps one of the earliest examples of a device used to teach a paced speaking pattern was the muthonome, also known as the "orthophonic lyre" for regulating the rhythm of speech in the treatment of stuttering. Developed by Colombat de l"Isere in 1830, the muthonome was similar to a mechanical metronome. Turning a key in the side of the spring-driven mechanical device wound the spring, providing the mechanical force for operation of the device. The rate of the muthonome's beats were controlled by sliding an owl-shaped weight along the length of a pendulum, much as is done with modern mechanical metronomes. This controlled how often a hammer inside the device struck the device's bell, which provided the "beat". Colombat felt that stuttering was caused by a lack of harmony between nervous activity and the musculature of the speech organs, and the muthonome was developed as a tool to restore the necessary physiologic harmony (from Wingate, 1976, pg. 154).

A more modern version, and one that was decidedly more portable than the muthonome, was the Pacemaster electronic metronome. In the middle of the 20th century, standard musician's mechanical metronomes were popular therapy tools. While effective in therapy settings in reducing the frequency of stuttering, they were too unwieldy and conspicuous to use in public. The Pacemaster was the joint development of E. Robert Libby, a stutterer, and 2 psychiatrists, Irwin Rothman and John Paul Brady (in later years Brady would write extensively about the use of psychotropic medication to treat stuttering). Both Rothman and Brady had used desk-top metronomes to treat stuttering, and Libby had good personal success with metronomically-paced speech. The Pacemaster marked their attempt to provide an inconspicuous portable metronome. It was first marketed in 1968. Residing in a standard "behind-the-ear" (BTE) hearing aid case, the device allowed control of volume and rate of the "beeping tones" emitted from the device into the earpiece. Users were encouraged to vary the metronome's beat rate on a frequent basis, to prevent adaptation and the loss of therapeutic effectiveness, a frequent problem noted with the use of metronomes.
Electronic metronomes were very popular therapeutic tools for stuttering in the 1960's and 70's and a wide variety of wearable devices were developed, with the Pacemaster only one example. A great deal of research supported the metronome's effectiveness (e. g., Wohl, 1968; Beech & Fransella, 1969; Brady, 1969; Greenberg, 1970; Berman & Brady, 1973). Several hypotheses have been proposed for the success of rhythmical or paced speech patterns in reducing the frequency of stuttering. These include the distraction effect, masking effect, the idea that a paced presentation allows better temporal ordering for the act of speaking, speaking to a superimposed rhythm simplifies motor planning requirements, and that the use of rhythmical speech reduces supersegmental aspects of speech production (reducing motor demands for speech production). Howell and El-Yaniv (1987) reported results for a different type of metronomic presentation that did not support the contention that rate pacing is vital part of the metronome's effectiveness. Howell and El-Yaniv used a metronome click that was triggered by user's own speech, rather then being presented continuously, and found it to have similar effectiveness in decreasing the frequency of stuttering.

There were many variations in the electronic metronomes. One of the most interesting was the Azrin, Jones, and Flye (1968) tactual electronic metronome. Like Shames and Torgeson's Vocaltech PVFD, the tactual metronome delivered rhythmic vibrotactile pulses, rather than auditory signals. The tactual metronome was primarily designed for research rather than daily use, so was somewhat cumbersome. The user wore a belt pack complete with standard size flashlight batteries and wires running to the pulsar unit, which was worn attached to the wrist. Another variation on the electronic metronome was provided by Donovan (1971). Donovan's device could be used to deliver a rhythmical tone, a continuous masking tone (for masked auditory feedback -- MAF), or a combined rhythmical pulsed masking tone.
Altered Auditory Feedback (AAF) Devices
Devices that alter the auditory feedback of the speaker's own voice are not new to the field of stuttering treatment. There has, however, been a recent surge of interest in these types of devices as technological advances and innovative designs and marketing techniques have captured both the consumers' and the clinicians' eye. Often referred to as altered auditory feedback (AAF) devices, they include those providing masked auditory feedback (MAF), delayed auditory feedback (DAF), frequency altered feedback (FAF), and those providing combinations of the various altered auditory feedback patterns (typically combined DAF & FAF). In a review paper on AAF and stuttering, Peter Howell has raised objections to the use of AAF to denote these types of devices, on the basis that the terminology assumes an active self-monitoring process in a negative feedback, compensatory pattern. He suggests using the term "alterations to recurrent auditory information" (ARAI) as it encompasses both feedback and non-feedback effects of alterations in the auditory environment of a speaker.
The reader is also referred to two excellent review articles in this subject area that appeared in earlier ISAD Online Conferences. Greg Snyder (2002) provided an extensive review of "The use of altered speech feedback in stuttering management" for the 5th International Stuttering Awareness Day Online Conference (ISAD5). Rick Merson (2003) provided "Auditory sidetone and the management of stuttering: from Wollensak to SpeechEasy", for the 6th International Stuttering Awareness Day Online Conference (ISAD6). Direct electronic links to both articles are provided in the References section of the present paper.
Masked auditory feedback (MAF)
Masked auditory feedback refers to the use of sound, generally a noise of some sort, of sufficient intensity to block the auditory feedback of the speaker's own voice to his or her ears. Of the three types of AAF, the effectiveness of MAF in reducing the frequency of stuttering was the first to be discovered. The early research appeared to come from Europe, in the late 1920's and early 1930's. (Van Riper, 1973, cites articles by Imhofer, 1927; Denes, 1931; and Kern, 1932). Interest appeared to wane, however, until the 1950's. Shane conducted experiments in the late 1940's on masking, evaluating the effectiveness of a 90 dB tone vs. that of a 25 dB tone at reducing the frequency of stuttering. Shane published the results of her experiments in 1955, beginning the modern era of interest in masking. From that point on, there was a rush of research to examine a variety of masking paradigms, including a variety of frequency and/or intensity permutations (e. g., Cherry and Sayers, 1956; Maraist & Hutton, 1957; Stromsta, 1958).
Early masking equipment tended to be laboratory-based and quite bulky, as well as requiring wall (AC) current for operation. Perhaps the earliest portable device was one developed by Derazne in 1959 in the Soviet Union. Called the Derazne Correctophone (Derazne, 1966), it was quite cumbersome, and required a large battery back carried in a knapsack to provide a portable power source. The user wore specially designed earphones to deliver the loud masking noise; the device had to switched off when the user wasn't speaking so that the conversational partner could be heard. Other early developers of portable models included Parker and Christopherson (1963), and Van Riper (1965).
A more modern and widely used electronic masking device was the Edinburgh masker.

The Edinburgh Masker was developed by Ann Dewar, a therapist at the Stammering Research Unit at Edinburgh University in Scotland, in conjunction with her husband, A. D. Dewar, a physician (Dewar, Dewar, Austin & Brash, 1979). The Edinburgh Masker consists of a throat microphone (held against the thyroid prominence by an elastic strap), a small control unit that can be worn on the belt or carried in a pocket, and either two separate earpieces or a headphone set. The masking noise is activated by phonation detected by the throat microphone; as soon as an utterance is completed and phonation stops, the lack of a throat microphone input signal automatically cuts off the masking noise. One challenge for these types of devices is individuals whose speech initiation is characterized by silent prolongations (blocks). Without input to the throat microphone, no masking is present to assist the user's speech. The control unit has a switch that allows manual activation of the masking noise for those occasions. The use of a throat microphone is an important feature for these types of devices; with a regular microphone, any conversation or environmental sound in close proximity to the microphone would cause the masking to be switched on, whether the user was speaking or not. The Edinburgh Masker reached the zenith of its popularity in the 1990s. Unfortunately, it is no longer manufactured. There are, however, other portable devices on the market that can be used to provide masking noise and can be paired with a throat microphone.
Delayed auditory feedback/DAF
Bloodstein (1993) relates an interesting anecdote as to how the delayed auditory feedback effect was discovered . . . . One day in or around 1950, an electronic engineer with the Signal Corps at Fort Monmouth, Bernard S. Lee, was trying out a new state-of-the-art tape recorder by recording his own voice. Included in the equipment was a set of headphones through which the operator could listen to a recording as it was being made. By error, Lee had plugged the headphones into the wrong jack. Through a peculiarity in the design of the device, this caused him to hear his recorded speech with a slight delay in the transmission, so that everything he heard in the headphones was what he had said a fraction of a second before. Under these conditions Lee, who is a normal speaker, found to his surprise that he was involuntarily repeating the first syllable of words. He was intrigued by this effect that he wrote an article "Artificial Stutter", and sent it to the Journal of Speech and Hearing Disorders, where it was published in 1951. . . . (p. 91).
The early research on DAF centered on its effect on normal speakers and how that would fit with various theoretical models of stuttering (e. g., Black, 1951; Lee, 1951; Fairbanks, 1955; Fairbanks and Guttman, 1958). The effect of DAF on the speech of normal speakers varied widely. Some individuals were unaffected by it, others were severely affected; for some it generated primarily sound prolongations, for others, repetitions, and for others, alterations in pitch, loudness, or even word finding. Of even more interest was the effect it had on individuals who stuttered. One of the earliest reports came from Nessel (1958) who reported that several stutterers became much more fluent while under DAF. Shortly thereafter, similar results were reported by others (e. g., Chase, Sutton, and Rapin, 1961; Lotzmann, 1961; Neelly, 1961). DAF has been applied in a variety of ways in therapeutic contexts. Goldiamond (1965) used DAF experimentally in an operant conditioning framework, using it as a punishment contingency to reduce stuttering, as well as a negative reinforcement contingency, and found success in both contexts. Webster and Lubker (1968) demonstrated that DAF also yielded successful results even when not applied contingently, by simply applying continuous DAF and noting a decrease in stuttering frequency. Ryan (1974) utilized DAF as a tool for reducing speech rate, and then gradually faded out the DAF. Shames and Florance (1980) used it as a tool to both slow the speech rate and to promote the use of sustained phonation (continuous voicing).
Possibly the newest DAF device to reach the market is the Defstut DAF device, from Great Britain (www.defstut.co.uk). Defstut consists of a small control unit that can be clipped to a belt or worn in a pocket, along with a separate lapel microphone and earphone set. The control unit also includes a switch that allows presentation of a low frequency masking tone. The MAF signal can be switched on when the speaker is experiencing a "silent block" and consequently DAF does not get activated (similar to the Edinburgh Masker described previously).
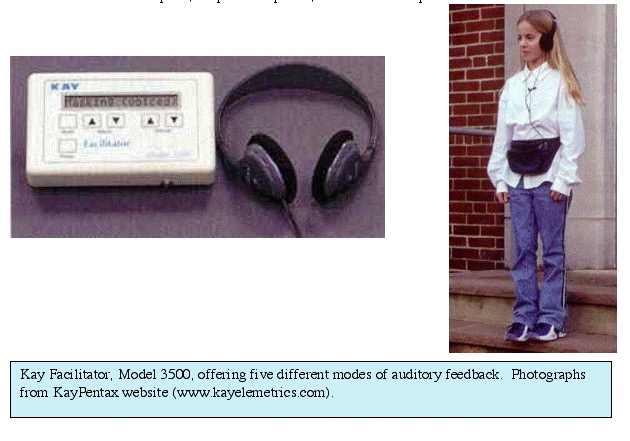
Today there are also a number of small portable devices on the market that provide DAF as one of several choices of AAF signals. The Kay Elemetrics Facilitator is one such device. The Facilitator was developed by Daniel Boone to be used with clients with a variety of communication disorders. It provides a choice of five alternative auditory patterns: DAF, MAF, an electronic metronome, amplified real-time auditory feedback, and a looping playback, so that the client immediately hear back what was just said. The device consists of a central control unit that can be worn in a belt pack, a lapel microphone, and a set of headphones.
Other auditory sidetones (frequency altered feedback/FAF)
The most recent of the altered auditory feedback modes to be introduced is frequency altered feedback, also known as frequency shifted feedback (FSF). The positive effect of FAF on decreasing the frequency of stuttering was first reported by Howell, El-Yaniv, and Powell (1987). In FAF conditions, the speaker's voice comes back in real-time, not delayed. It is, however, electronically shifted in frequency by the FAF device. The effects of FAF in stutterers has been examined in a variety of paradigms, including frequency shifting in either direction, at various speaking rates, etc. (e. g., Howell, El-Yaniv, & Powell, 1987; Howell, Wingfield, & Johnson, 1988; Kalinowski, Armson, Roland-Mieszkowski, Stuart, & Gracco, 1993; Kalinowski, Stuart, Rastatter, Miller, Zimmerman & Shine, 1998).
One of the earliest of the commercially-marketed FAF devices was the Fluency Master, developed by Ron Webster (Webster, 1991) at the Hollins Communication Research Institute (HCRI). The device, which was introduced in 1992, no longer has any ties to HCRI. The Fluency Master's electronic circuitry and battery is housed in a behind-the-ear (BTE) hearing aid style case. Extending from the base of the BTE case on a electrical wire tether is the microphone, in this case a vocal pick-up device that sits atop the mastoid process of the temporal bone and which responds to bone and tissue-conducted speech. The mastoid apparatus gives the Fluency Master a more unwieldy and more cosmetically conspicuous appearance than the SpeechEasy hearing aid style devices (to be discussed later), however, the arrangement has a strong advantage. It primarily only responds to the user's voice, rather than altering all the environmental sounds picked up by the case mounted microphones of the SpeechEasy devices. The exact operating and FAF characteristics of the Fluency Master device are unclear. Richard Merson, in his 2003 ISAD paper on AAF devices (mentioned earlier) suggests that the device may also produce an undocumented DAF effect, possibly by virtue of it's signal processing paradigm. A photograph of the Fluency Master appears below.

Combined/Multiple Feedback Devices (DAF/FAF/MAF)
There are several rationales that underlie the various devices that offer two or more choices of altered auditory feedback. Some researchers feel that the use of two feedback modes (DAF and FAF) will prevent the user adapting to the feedback and experiencing gradually diminishing effectiveness (e. g., MacLeod, Kalinowski, Stuart, & Armson, 1995; Kalinowski, Stuart, Rastatter, Miller, Zimmerman, & Shine, 1998). Other clinicians and/or manufacturers go with combination devices to offer the user a greater degree of choice in selecting which feedback mode or modes to use.
By far the largest number of modern assistive devices for the treatment of stuttering lie in this "AAF combination" category, and they vary widely in features. One manufacturer, Casa Futura Technologies, was among the first to offer a variety of AAF devices. Its most recent offering is an upgrade of the company's Pocket Fluency System, now called the Pocket Speech Lab (PSL). The PSL offers DAF and FAF that can be delivered independently or simultaneously, and a switch on the side of the control unit that can be pressed to deliver MAF in the case of occurrence of "silent blocks" (as discussed previously). The PSL also offers a "vocal tension biofeedback" component that can interface with the AAF components, switching them on and off (discussed previously). The PSL consists of a small control unit that clips on the belt or fits in a pocket, and a variety of headset and microphone options. These include cell phone-style unitary earphone & microphone units, lapel microphones, several choices of throat microphones (at an additional cost), headphones, and wireless headset/microphone combinations. A photograph of the Pocket Speech Lab appears below. The National Center for Stuttering also sells a device that appears to be very similar to Casa Futura's Pocket Fluency System.

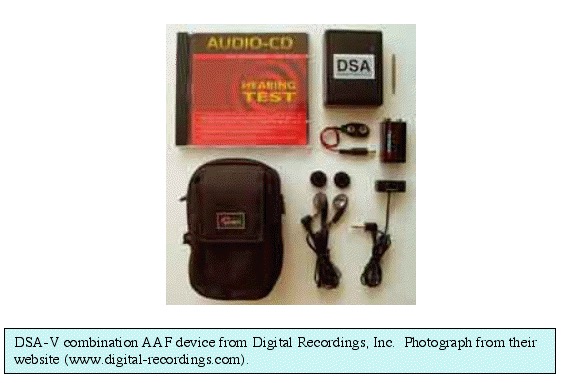
In Europe, Marek Roland-Mieszkowski, Andrzej Czyzewski, and Bozena Kostek developed a combination AAF device, the Digital Speech Aid (DSA). Their prototype device was introduced in 1992, and they examined the effectiveness of several different feedback modes, including FAF, MAF, combined DAF & FAF, and two "discorrelative feedback" modes. Now in its 5th generation, the DSA-V consists of a small control unit (pocket, belt, or arm-band mountable), lapel microphone, and walkman-style ear bud earphones. The device is marketed through Digital Recordings, Inc, located in Nova Scotia, Canada.
Michael Rastatter, Joseph Kalinowski and Andrew Stuart, and several of their colleagues and graduate students at East Carolina University carried out extensive research on AAF effects over the last decade. The University patented its design for hearing aid-style AAF devices in 1999. The devices are marketed by Janus Development Group. There are three Speech Easy AAF devices: a "behind-the-ear" (BTE) version, an "in-the canal" (ear canal) (ITC) version, and a "completely-in-canal" (CIC) version. All three provide simultaneous DAF and FAF. Both basic and advanced models are available, and some versions can be fitted with add-on components, such as a dual memory setting that allows to user to switch between AAF processing when speaking is necessary and unaltered auditory feedback when the user will be listening but not speaking. All of the components necessary for an AAF device (microphone, control/processing unit, and speaker/earphone) are miniaturized and fit inside the hearing-aid style cases. A photograph of the SpeechEasy devices appears below.

Miscellaneous Devices
Anxiety and Fear-Reducing Devices: It would be a shame to end this paper without mentioning at least one more class of assistive devices, and a rather unique device that falls within that category. Anxiety, towards stuttering, towards speaking situations, towards feared sounds and feared words, can be a major component of the disorder for many people who stutter. Several laboratory instruments have been utilized in the past to measure physiologic correlates of anxiety, such as Palmar Sweat Indexes (PSI) and Galvanic Skin Response (GSR). These devices typically were used to obtain research measurements, but were not used as clinical devices, and so were not included in this paper. A few years ago, Casa Futura Technologies introduced a device that had been suggested for use in treating Post-Traumatic Stress Disorders (PTSD). One controversial technique for treating PTSD is "Eye Movement Desensitization and Reprocessing" (EMDR) therapy. According to the developer of the EMDR treatment device, in EMDR therapy, clients are asked to describe their traumatic experiences. If the client feels any anxiety or discomfort, they are asked to rate the degree of discomfort. Clients are then instructed to gaze to the extreme left side of their visual field, then follow the psychotherapist's finger, moving their gaze to the extreme right side of the visual field. This pattern of alternating gaze is repeated 24 times. It has been reported that ratings of discomfort towards the traumatic event often drop dramatically after an eye movement sequence. Casa Futura Technologies developed a pair of sunglasses to allow stutters to self-conduct EMDR eye-movement sequences if they were feeling anxious upon coming upon a feared word and beginning to stutter. On the inside of the sunglass frame was a line of LEDs (lights). Attached to the glasses was a wire leading to a control unit, held in the hand or pocket. Upon feeling anxiety and beginning to stutter, the user would press the control unit button and the lights would begin moving sequentially towards the left corner, then the right corner, then back to the left, etc. The user would pause in their speech, follow the gaze cues provided by the lights until the sequence was completed, then resume speaking, albeit at a greatly reduced anxiety level. There is little information available concerning how successful the glasses were at reducing anxiety and thus reducing the frequency of stuttering, and the glasses are not currently being marketed. Yet the device, as do many of the other ones discussed in this paper, certainly demonstrates the level of interest in alternative therapies to treat stuttering, and the creative ways in which technology has been approached.

In closing our review of various assistive devices that have been employed in treating stuttering, it might be a good idea to leave the reader with a parting gift. For anyone considering the use or purchase of a treatment procedure, product, or program, the American Speech-Language-Hearing Association provides the following suggestions:
- What are the stated uses of the product?
Should be clearly specified - To which client/patient population does it apply?
Is there documented evidence that it is valid for use with a specified population? - Are the outcomes clearly stated?
Expected outcomes should be available with supporting data - What published material is available?
Is promotional material the only published source of information? - Is there peer-reviewed research that supports or contradicts promotional claims?
Quality and quantity of research should be considered - What is the professional background of the developers?
Knowledge, expertise, and experience - Availability & Cost: are other options available, and if so, how do they compare?
Is the product the best choice in terms of documented performance and benefits - Experience: have you talked with others who have experience with this product?
Source of valuable insights into actual use - Is it within my profession's Scope of Practice?
ASHA Code of Ethics requires members to only do what they are trained and competent to do - Are there ASHA statements or guidelines on this topic?
Policy documents may assist in decision making - Based on the above factors, is the cost reasonable and justifiable?
Additional Questions:
- What are potential risks/adverse consequences?
- What are the potential benefits?
- What is recommended as sufficient training to be a qualified user of the product/procedure?
- Is it FDA registered and/or approved (if so required)?
- What training & technical support are available?
- Is there a guarantee or return policy?
- Are there contraindications for specific populations or etiologies?
Azrin, N., Jones, R. J., & Flye, B. (1968). A synchronization effect and its application to stuttering by a portable apparatus. Journal of Applied Behavioral Analysis, 1(4), 283-295.
Basmajian, , J. V. (1972). Electromyography comes of age. Science, 176, 603-609.
Beech, H. R. & Fransella, F. (1968). Explanations of the rhythm effect in stuttering. In Gray, B. B. & England, G. (Eds.), Stuttering and the Conditioning Therapies. Monterey: The Monterey Institute for Speech and Hearing.
Berman, P. A & Brady, J. P. (1973). Miniaturized metronomes in the treatment of stuttering: A survey of clinician's experiences. Journal of Behavioral Therapy and Experimental Psychiatry, 4, 117-119.
Black, J. (1951). The effect of sidetone delay upon vocal rate and intensity. Journal of Speech and Hearing Disorders, 16, 56-60.
Bloodstein, O. (1993). Stuttering: The Search for a Cause and Cure. Boston: Allyn and Bacon.
Bloodstein, O. (1995). A Handbook on Stuttering (5th Edition). San Diego: Singular Publishing.
Bogue, B. N. (1919). Stammering: Its Cause and Cure. Indianapolis: Wm. B. Burford, Pub.
Brady, J. P. (1968). A behavioral approach to the treatment of stuttering. American Journal of Psychiatry, 125(6), 843-848.
Brady, J. P. (1969). Studies of the metronome effect on stuttering. Behavioral Research and Therapy, 7(2), 197-204.
Chase, R. A., Sutton, S., & Rapin, I. (1961). Sensory feedback influences on motor performance. Journal of Auditory Research, 1, 212-223.
Cherry, E. C. & Sayers, B. M. (1956). Experiments on the total inhibition of stammering by external control, and some clinical results. Journal of Psychodynamic Research, 1, 233-246.
Cross, D. E. (1977). Effects of false increasing, decreasing, and true electromyographic biofeedback on the frequency of stuttering. Journal of Fluency Disorders, 2(2),109-116.
Derazne, J. (1966). Speech Pathology in the U.S.S.R. In Rieber, R. W. & Brubaker, R. S. (Eds.), Speech Pathology. Amsterdam: North Holland.
Dewar, A., Dewar, A. D., Austin, WTS., & Brash, H. M. (1979). The long-term use of an automatically triggered auditory feedback masking device in the treatment of stammering. British Journal of Disorders of Communication, 14, 219-229.
Donovan, G. E. (1971). A new device for the treatment of stuttering. British Journal of Disorders of Communication, 6(1), 86-88.
Fairbanks, G. (1955). Selected vocal effects of delayed auditory feedback. Journal of Speech and Hearing Disorders, 20, 333-345.
Fairbanks, G. & Guttman, N. (1958). Effects of delayed auditory feedback upon articulation. Journal of Speech and Hearing Research, 1, 12-22.
Friedman, A., Fetterman, E., and Jolson, Y. (1999). Dr. Fluency Computerized Stuttering Treatment Program User's Guide (Version 2.3). Jerusalem, Israel: Speech Therapy Systems, Ltd.
Goebal, M. D. (1994). CAFET Program. Annandale, VA: Annandale Fluency Clinic.
Goldiamond, I. (1965). Stuttering and fluency as manipulatable operant response classes. In Krasner, L. & Ullman, L. P. (Eds.) Research in Behavior Modification. New York: Holt, Rinehart, Winston.
Greenberg, J. B. (1970). The effect of the metronome on the speech of young stutterers. Behavioral Therapy, 1(3), 240-244.
Guitar, B. (1975). Reduction of stuttering frequency using analog electromyographic feedback. Journal of Speech and Hearing Disorders,18(4), 672-685.
Hanna, R., Wilfling, F., & McNeil, B. (1975). A biofeedback treatment for stuttering. Journal of Speech and Hearing Disorders,18(2), 270-273.
Hargrave, S., Kalinowski, J., Stuart, A., Armson, J., & Jones, K. (1994). Effect of frequency altered feedback on stutterers' fluency at two speech rates. Journal of Speech and Hearing Research, 37, 1113-1119.
Howell, P. & El-Yaniv, N. (1987). The effects of presenting a click in syllable-initial position on the speech of stutterers: Comparison with a metronome click. Journal of Fluency Disorders, 12, 249-256.
Howell, P., El-Yaniv, N. & Powell, D. J. (1987). Factors affecting fluency in stutterers when speaking under altered auditory feedback. In Peters, H. & Hulstijn, W. (Eds.), Speech Motor Dynamics and Stuttering. New York: Springer-Verlag.
Howell, P., Wingfield, T., & Johnson, M. (1988). Characteristics of the speech of stutterers during normal and altered auditory feedback. In Ainsworth, W. A. & Holmes, J. N. (Eds.), Proceedings Speech 88, Vol. 3, (7th Federation of Acoustical Societies of Europe Conference). Edinburgh: Institute of Acoustics.
Kalinowski, J., Armson, J., Roland-Mieszkowski, M., Stuart, A., & Gracco, V. (1993). The effects of alterations in auditory feedback on stuttering frequency. Language and Speech, 36, 1-16.
Kalinowski, J., Stuart, A., Rastatter, M., Miller, R., Zimmerman, S., & Shine, R. (1998). Examination of altered auditory feedback: Therapeutic implications. In E.C. Healey, & H.F.M. Peters (Eds.), Proceedings from the Second World Congress on Fluency Disorders (pp. 54-57). Nijmegen, The Netherlands: University Press Nijmegen.
Lanyon, R. I. (1977). Effect of biofeedback-based relaxation on stuttering during reading and spontaneous speech. Journal of Consulting and Clinical Psychology, 45(5), 860-866.
Lee, B. S. (1951). Artificial stutter. Journal of Speech and Hearing Disorders, 16(1), 53-55.
Lewis, G. A. (1897). The Origin and Treatment of Stammering. Philadelphia: The Lewis Phono-Metric Institute.
Lotzmann, G. (1961). On the use of varied delay times in stammerers. Folia Phoniatrica, 13, 276-310.
Maraist, J. A. & Hutton, C. (1957). Effects of auditory masking upon the speech of stutterers. Journal of Speech and Hearing Disorders, 22(4) 385-392.
MacLeod, J., Kalinowski, J., Stuart, A., & Armson, J. (1995). Effect of single and combined altered auditory feedback on stuttering frequency at two speech rates. Journal of Communication Disorders, 28, 217-228.
Merson, R M. (2003). Auditory sidetone and the management of stuttering: from Wollensak to SpeechEasy. 6th International Stuttering Awareness Day Online Conference (ISAD6). Link: http://www.mnsu.edu/comdis/isad6/papers/merson6.html
Neelly, J. N. (1961). A study of the speech behaviors of stutterers and non stutterers under normal and delayed auditory feedback. Journal of Speech and Hearing Disorders Monograph, 7, 63-82.
Nessel, E. (1958). Die verogerts sprachruckklopplung (Lee-effect) bei der stotterern. Folia Phoniatrica, 10, 199-204.
Parker, C. S, and Christopherson, F. (1963). Electronic aid in treatment of stammer. Medical Electronics and Biological Engineering, 1(2), 121-125.
Potter, S. O. L. (1882). Speech and Its Defects. Philadelphia: Blakiston.
Ryan, B. F. (1974). Programmed stuttering therapy for children and adults. Springfield: C. C. Thomas.
Shames, G. H., & Florance, C. L. (1980). Stutter-Free Speech: A Goal for Therapy. Columbus, OH: Merrill.
Shames, G. H., & Wiig, E. H. (1990). Human Communication Disorders (3rd Edition). Columbus: Merrill.
Shane, M. L. S. (1955). Effect on stuttering of alteration in auditory feedback. In Johnson, W. (Ed.), Stuttering in Children and Adults. Minneapolis: University of Minnesota Press.
Snyder, G. (2002) The use of altered speech feedback in stuttering management. 5th International Stuttering Awareness Day Online Conference (ISAD5). Link: http://www.mnsu.edu/comdis/isad5/papers/snyder.html
Stromsta, C. (1958). The effects of altering the fundamental frequency of masking on the speech performance of stutterers. Technical Report, National Institutes of Health, Project B-1331.
Treon, M., & Tamayo, F. M. V. (1975). The separate and combined effects of GSR biofeedback and delayed auditory feedback on stuttering: A preliminary study. Journal of Fluency Disorders, 1(1),2-9.
Van Riper, C. (1965). Clinical use of intermittent masking noise in stuttering therapy, Asha, 7, 381.
Van Riper, C (1973). The Treatment of Stuttering. Englewood Cliffs, NJ: Prentice-Hall. Webster, R. L. & Lubker, B. B. (1968). Interrelationships among fluency-producing variables in stuttered speech. Journal of Speech and Hearing Research, 11, 754-766.
Webster, R. L. (1980). Precision Fluency Shaping Program: Speech Reconstruction for Stutterers. Blacksburg, VA: University Publications/Physical Biological Sciences Ltd. For Communications Development Corp.
Webster, R. L. (1991). Manipulation of vocal tone: Implications for stuttering. In Peters, H., Hulstijn, W., & Starkweather, C. W. (Eds.), Speech Motor Control and Stuttering. Amsterdam: Elsevier-Science.
Wingate, M. E. (1976). Stuttering: Theory and Treatment. New York: John Wiley and Sons
Wingate, M. E. (1997). Stuttering: A Short History Of A Curious Disorder. Westport, CT: Bergin and Garvey.
Wohl, M. (1968). The electronic metronome an evaluative study. British Journal of Disorders of Communication, 5(1), 66-76.
October 1, 2005